LITERATURE - 2021, Journal of Hungarian Obstetricians and Gynaecologists
Shoulder Dystocia

Author: Petru Chitulea MD1, Cristian Cheta MD2, Tania Negru3
1Associate professor Faculty of Medicine University of Oradea, Head of the clinical department of the Oradea County Emergency Clinical Hospital - Maternity
2Oradea County Emergency Clinical Hospital - Maternity
3Medical Student of Medicine University of Oradea
Shoulder dystocia is one of the most dramatic events in obstetrics and represents the blockage of the shoulders after the expulsion of the fetal skull. This rare but even more dramatic phenomenon, especially when not foreseen, will deeply mark the obstetrician for the rest of his life. For this reason, the professional training of the obstetricians must include a proper preparation for this emergency situation. It is hard to imagine for those who have not experienced such an obstetrical complication the degree of stress and drama of shoulder dystocia that appeared unexpectedly in expulsion. As in general in medicine, prevention is the best attitude, treating this obstetric accident is difficult, risky and burdened by maternal and fetal complications.
Keywords: macrosomia, shoulder dystocia, obstetric maneuvers, elective cesarean section
Etiology
The main cause of shoulder dystocia is fetal macrosomia, fetuses over 4000 g, and according to some authors over 4500 g estimated antepartum weight. The most common maternal causes of fetal macrosomia are obesity, diabetes, and genetic factors. Other factors that can lead to shoulder dystocia is postterm pregnancy with low amniotic fluid volume, due to lack of lubrication.
Frequency
The frequency of shoulder dystocia in the case of fetuses over 4000 g is 7% and the incidence is 22 times higher in the case of fetuses over 4500 g. Reporting the incidence of shoulder dystocia varies widely in the literature, but it is accepted that the incidence has increased significantly over the past decades do the increasing incidence of macrosomal fetuses.
Mechanism of production
In fetal macrosomia, especially for fetuses over 4500 g, has as a consequence a thoracic, abdominal and biacromial perimeter larger than the diameters of the fetal skull, so after the expulsion of the skull the shoulders become blocked at the upper strait. The arms also leads to higher thoracic volume and when the diameters of the pelvis are smaller than it, the fetal rotation can be blocked; the rotation of the shoulders in an oblique diameter is more favorable.
Another factor that contributes to shoulder dystocia is the retraction of the cervix relatively quickly on the fetal neck after the expulsion of the skull, which aggravates the situation, therefore obstetric maneuvers must be started immediately and competently, time is an important and critical factor for success.
Consequences
Fetal consequences
Shoulder dystocia is sometimes accompanied by violent uterine contractions (the uterus fights against the obstacle) which can lead to fetal hypoxia by compression of the umbilical cord and / or premature placental abruptio with the appearance of placental hematoma. In such situations the cyanosis of the expelled fetal head is observed and its blockage in the pubic occipito in such a way that the fetal airways are blocked in the posterior perineum makes their aspiration difficult or impossible. If the situation is prolonged, the fetus will suffer hypoxic brain damage until fetal death.
The practical consequence of this is that the clamping and sectioning of the umbilical cord are contraindicated even in the case of a pericervical cord circumference and when obstructive maneuvers to release the shoulders succeed, fetal resuscitation should be performed with the umbilical cord unthinkable for at least 1-2 minutes because the fetus can recover the blocked blood in the placenta.
About 30% of children born with dystocia of the shoulders have late neuropsychiatric dysfunction and about 40% of them have immediate morbidity. Also, fetal brachial plexus lesions are relatively common and can evolve up to permanent upper limb paralysis, being accompanied or not by deliberate or untimely clavicular fractures.
Maternal consequences
Obstetric maneuvers performed sometimes with force can lead to injuries of the birth canal: rupture of the cervix, vaginal wall, traumatic injuries of the bladder and urethra, debilitating ruptures of the posterior perineum and sometimes this can affect the anus and rectal wall.
Accidental or iatrogenic pubic symphysis lesions (symphysiotomy) may also occur. The most dramatic accident that can occur due to the combination of violent uterine contractions with internal and external maneuvers is uterine rupture.
In the case of intrapartum fetal death, for fetal extraction, scarf embryotomy should be performed, with all its inherent risks, cesarean section in this case unjustifiably supplementing the maternal trauma.
Attitude
Attitude regarding obstetrical behavior in the case of fetal macrosomia there are two situations:
- Monitored pregnancies, when we can estimate the fetal weight.
- Unmonitored pregnancies, first presentation in Obstetrics Department is during labor or even expulsion, like a "surprise in the delivery room".
In first situation, I consider that in the vast majority of cases (depending on the parity, maternal pelvis and pregnancy associated pathology), the delivery should happen by scheduled cesareansection as an optimal solution to prevent severe maternal-fetal outcomes. I came to this conclusion after a long experience that taught me that it is almost impossible to predict all the factors involved in the birth process and the risk-taking by the obstetrician is unacceptable given the fetal and maternal consequences of shoulder dystocia. Thus, the healing of a symphysiotomy or the vaginal ruptures propagated in the rectum, as well as the bladder and urethral lesions are much harder to cure than a cesarean section, producing long-lasting maternal sequelae, sometimes for the rest of life.
In the case of unmonitored pregnancies when the childbirth reaches labor or expulsion in the delivery room, there are several situations that can indicate the increased risk of shoulder dystocia: prolonged time of birth and/or expulsion and the need to apply a forceps to the middle strait in the case of obese patients are good indicators of the imminence of shoulder dystocia, also the correct attitude in this situation is the termination of birth by caesarean section.
If the drama has already occurred (skull expelled and shoulders blocked in the pelvis) we have several obstetric techniques with a reasonable efficiency. It should be emphasized that the speed of execution of these interventions is essential, time is a critical factor for installation of fetal hypoxia therefore this techniques must be learned and practiced in advance by the obstetric team. Training of these maneuvers is important to reduce the reaction time as much as possible and to prevent panic in the delivery room.
Obstetric techniques in shoulder dystocia
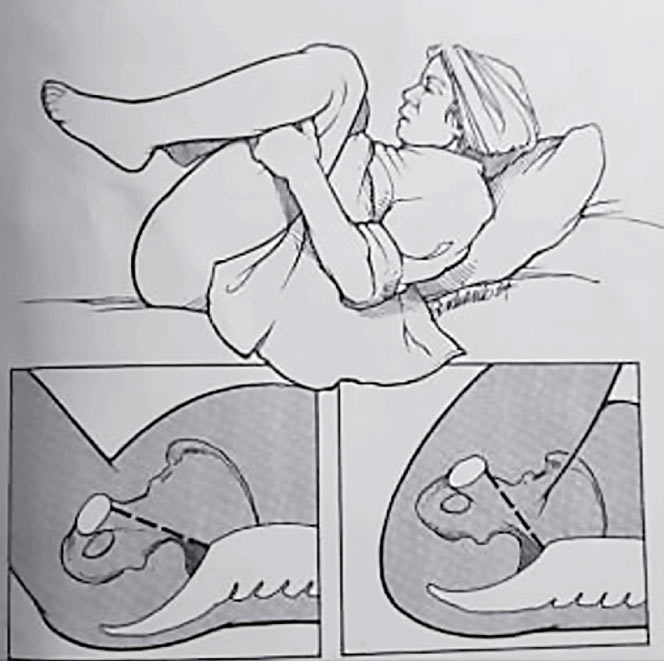
The McRoberts maneuver
The McRoberts maneuver (Figure 1) is a simple, logical technique that in average cases ensures the birth of the shoulders and involves the hyperflexion of the maternal thighs on the abdomen which leads to a flattening of the lumbar spine and a ventral rotation of the pelvis and maternal pubic symphysis. This maneuver can be combined with the sustained expulsive effort of the parturition with the gentle support of the uterine fundus (The Krissteller maneuvers in force are contraindicated). Gentle suprapubic compression which facilitates the release of the anterior shoulder may also be helpful.
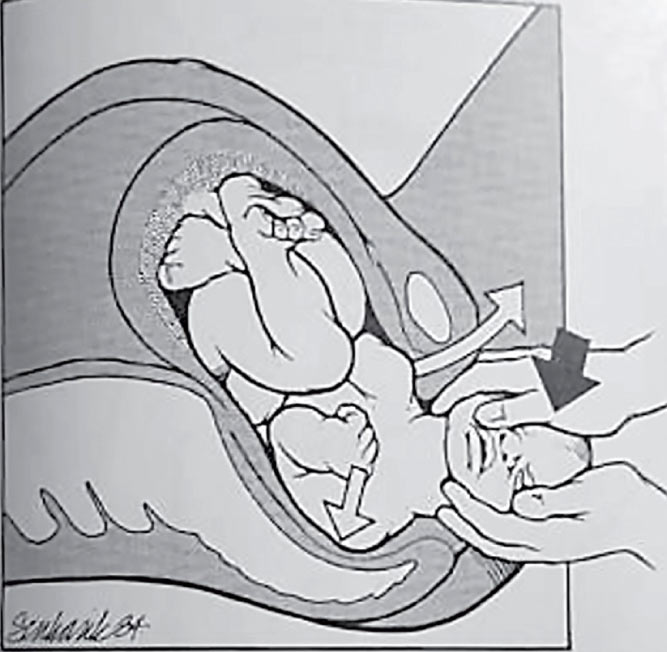
Attempts to rotate the fetal skull should be avoided, but the fetal skull can be raised and lowered gently to facilitate shoulder engagement (Figure 2). If this maneuver fails, the obstetrician can insert a hand behind the fetal occiput into the vagina by pushing the anterior shoulder below the symphysis into an oblique diameter. In any case, traction on the fetal skull must be avoided, although this is the tendency and the natural reaction of the obstetrician which face of unexpected and dramatic situations.
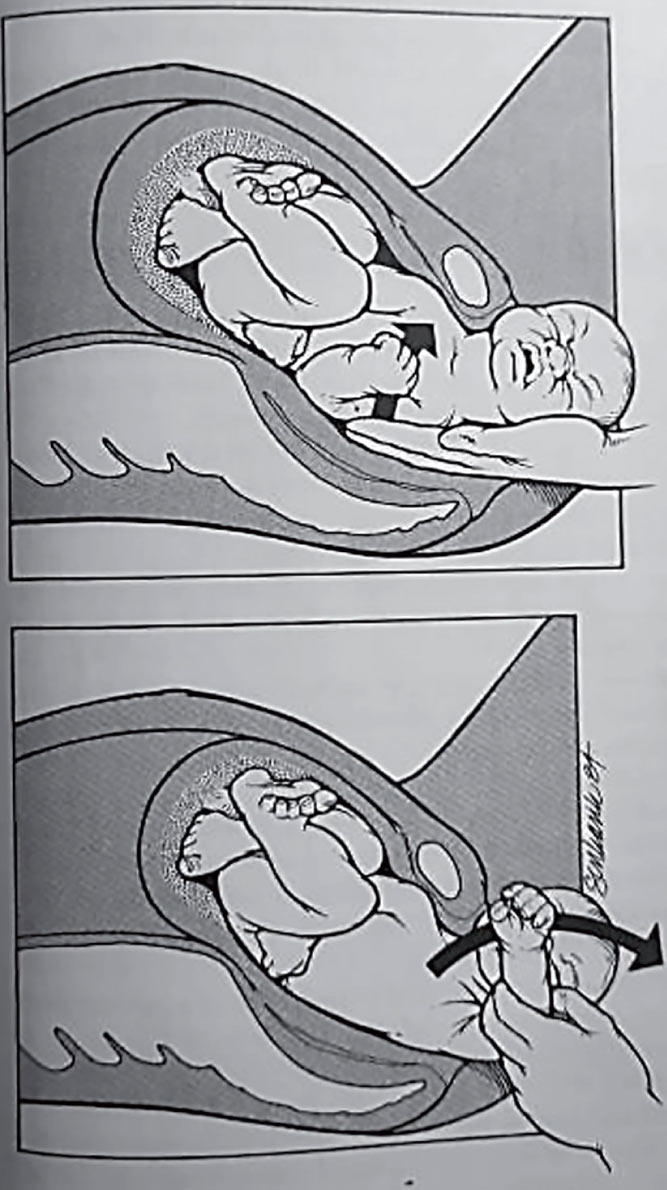
Wood screw maneuver
Another possible technique is the "wood screw maneuver" (Figure 3) the back shoulder can be rotated forward by 180 degree by passing it under the pubic symphysis. Some authors recommend the birth of the posterior arm by inserting the operator's hand into the vagina up to the elbow of the fetus after which it is flexed and extracted on the front of the fetal breast. This maneuver can lead to the fracture of the fetal humerus, but it heals without consequences, being preferable to the brachial plexus injury, which can lead to a permanent disability.
Cleidotomy
Deliberate fracture of the collarbones is a heroic maneuver but necessary when the other maneuvers fail. Cleidotomy is always performed digitally, gently, avoiding fetal lesions of the pleural dome. The clavicle fracture occurs "in green wood", the purpose of this maneuver is to reduce the fetal bi-acromial diameter, following the healing without consequences is the rules. It is advisable to bill both clavicles to sufficiently reduce the biacromial diameter without producing an accentuated displacement of a clavicle towards the pleural dome.
Zavanelli maneuver
In the USA in case of uncorrected or difficult to correct shoulder dystocia, the fetal skull is pushed and supported in the uterus by other helper followed by emergency cesarean section.
Subcutaneous symphysiotomy
This technique rarely used, which according to the literature seems to be effective in desperate situations, performed quickly without waiting too long (thus avoiding hypoxia and fetal acidosis) but with which, personally, I have no experience.
Conclusions
Shoulder dystocia is not always easy to predict but the correct analysis of the risk factors of fetal macrosomia as well as maternal risk factors, combined with fetal ultrasound parameters can lead to a reasonable estimate of its risk.
In my opinion, heroic and sometimes brutal obstetric maneuvers must be reserved for cases in which dystocia could not be predicted (surprise in the delivery room) as they always have a high degree of unpredictability of their efficiency. That is why I consider that, as in the case of other obstetric accidents, the best attitude is prevention and in case of doubt, elective cesarean section is the optimal solution. Moreover, forcing all obstetricians, through professional guides, to perform heroic obstetric maneuvers, difficult to learn, and especially difficult to perform correctly in a factual situation rarely encountered in the current practice of smaller hospitals; of maximum stress, and anyway with uncertain outcome, opens wide the gate of mall praxis accusations against them. If in the large university clinics with a significant number of thousands of births per year, equipped with all modern medical logistics, but especially with a specialized medical staff, who had the opportunity to gain solid experience solving dramatic obstetric situations, the temptation to give birth on vaginal route of macrosomal fetuses, in carefully selected cases, may be an option, in the case of most medium and small hospitals, this in my opinion, should be avoided.
The assumption by the obstetrician who assists a birth with a macrosome fetus of the possible fetal and maternal risks of a possible shoulder dystocia I consider being an ethically questionable approach.
This article, far from being an objective meta-analysis of the literature on the field of shoulder dystocia, is rather my objective personal opinion, based on a long practical experience.
At the end, I can't conclude without quoting my mentor Acad. Prof. Dr. Ioan Munteanu who, concluding the works of the International Congress of Obstetrics-Gynecology of the DKMT Euroregion oct. 2004 which he chaired, he said “a better an extra cesarean section than a disabled child furthermore”.
Selective Bibliography
- Williams Obstetrics, 25th Edition
- Pocket Companion to obstetrics, normal & problem pregnancies, 3th Edition
- SROG - professional guides
- Gherman RB, Tramont J, Muffley P, Goodwin TM. Analysis of McRoberts' maneuver by x-ray pelvimetry. Obstet Gynecol 2000; 95: 43-7.
- Gobbo R, Baxley EG. Shoulder dystocia. In: ALSO: advanced life support in obstetrics provider course syllabus. Leawood, Kan.: American Academy of Family Physicians, 2000.
- Stallings SP, Edwards RK, Johnson JW. Correlation of head-to-body delivery intervals in shoulder dystocia and umbilical artery acidosis. Am J Obstet Gynecol 2001; 185: 268-74.
- Boulvain M, Stan C, Irion O. Elective delivery in diabetic pregnant women. Cochrane Database Syst Rev 2003; 2: CD001997.
- Lam MH, Wong GY, Lao TT. Reappraisal of neonatal clavicular fracture: relationship between infant size and neonatal morbidity. Obstet Gynecol 2002; 100: 115-9.
Download Full Article
- Petru Chitulea: Shoulder Dystocia (2021, Journal of Hungarian Obstetricians and Gynaecologists, PDF, 4 pages, English, 1.26MB)