LITERATURE - 2017, Journal of Hungarian Obstetricians and Gynaecologists
Successfully treated case of a patient with giant benign ovarian tumor and suicide attempt

Authors: Tibor Novák MD1, László Andrási MD2, Zsolt Szabó MD3, Gábor Németh MD1
University of Szeged 1Department of Obstetrics and Gynecology (director: Gábor Németh MD, Med. Habil.);
2Department of Sugery (director: György Lázár MD);
3Department of Anaesthesiology and Intensive Therapy (director: Zsolt Molnár MD)
The case of a patient with giant ovarian tumor was presented, who was referred to have planned laparotomy because of an enormous intraabdominal mass found during gynecological examination, a few day before her admission to the emergency care unit. The particularity of this case was the patient’s attempted suicide using a high dose of an antihypertensive drug. At the moment of the admission, this important information was obtained from the relatives. Finally, in the recovery period, the patient confirmed this information; she said she had made the attempt because „she was exhausted”.
Keywords: giant ovarian tumor, suicide attempt
A 56-year-old woman with a huge intraabdominal mass presented at the emergency care unit as she had a suicide attempt using a high-dose of lercanidipine based tablets. On admission, her regular medications were allopurinol 300 mg/day, ropinirole 4 mg/day, levodopa 100–50–200 mg/day, alprazolam 0.5 mg/day, pantoprazole 2x40 mg/day, spironolactone 25 mg/day, furosemide 1 tablet/day, and potassium chloride 1 capsule/day. The patient had a history of spondylosis, arthrosis, generalized depression, incipient Parkinson’s disease, and urinary incontinence. Some decades before she had undergone an ovarian cyst extirpation, and for about 20 years, she had worked with chemical agents in horticulture.
Rapidly deteriorating cardio-respiratory parameters, aspiration of gastric juice, clinical signs of right-sided pneumonia, need for assisted ventilation and compression of the intraabdominal organs due to a giant multifocal left ovarian cyst were observed. The preoperative status is presented in Figure 1.
After the stabilization of the vital parameters by the Intensive Care Unit (ICU) members, urgent median laparotomy was performed. As an initial step, the content of the cyst was aspirated for better mobilization of the tumor. Approximately 24 litres of bloody stained, cloudy liquid were removed during the process.
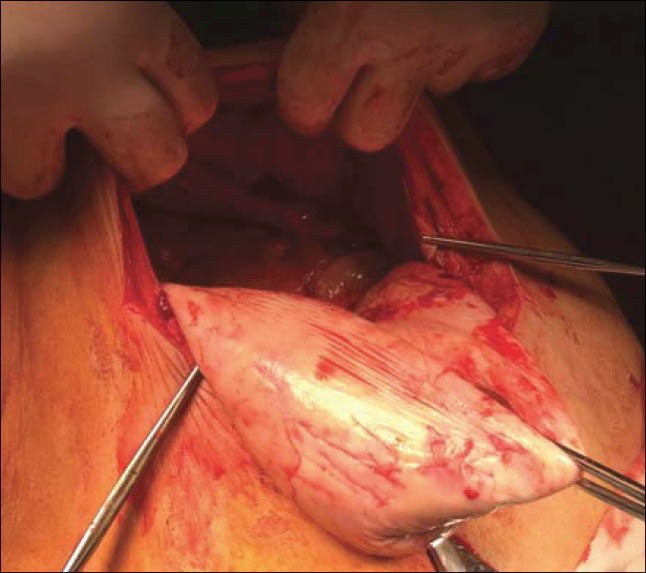
After that, a step-by-step adhesiolysis was necessary because of the massive adhesions between the intraabdominal organs, peritoneum and the surroundings of the cyst. The internal genitalia were identified and removed: first the left adnexa, followed by the uterus together with the right adnexa. An intrauterine contraceptive device was found. The total amount of the fluid removed from the multicystic tumor was about 26 L. Intraoperative image before the removal of the left adnexa is presented in Figure 2.

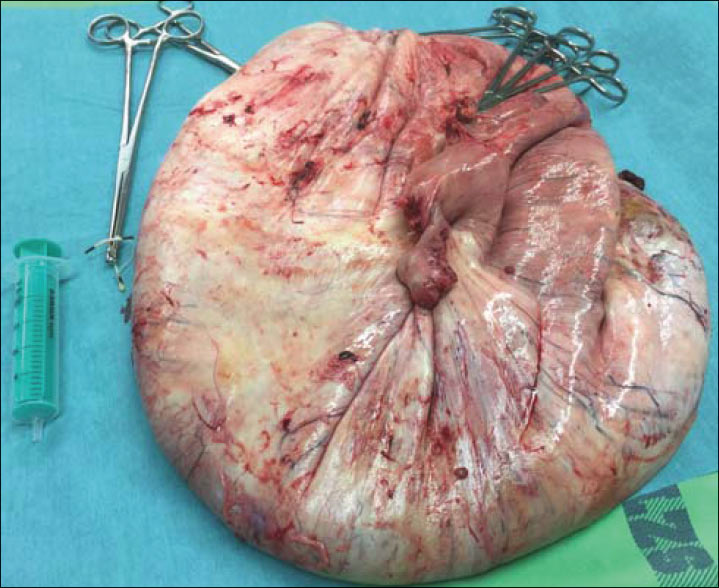
The histopathological examination performed later showed a serous ovarian cystadenoma without signs of atypia or malignancy. The weight of the eliminated mass was about 30 kg (see Figure 3.) During separating the mass from the surrounding structures, hemodynamic deterioration was noticed as a consequence of significant diffuse bleeding. It was managed surgically, with the need of massive blood transfusion, volume replacement, and inotropic therapy.
In the postoperative period, there were no signs of intraabdominal complications. A tracheostoma was implanted, and for different types of bacterial and fungal infections and dermatological abnormalities on the lower extremities, the adequate therapeutic measures were made (antibiotics and antifungal treatment, and local topical therapy). The patient’s health status improved gradually, the abdominal drains were removed, bowel movements and stool formation were recorded, and oral feeding was initiated. She was discharged from the ICU on the 18th postoperative day and was transferred for the rehabilitation.
In this period, due to a hemodynamic instability causing hematochezia, colonoscopy was performed, but only a colonic diverticulosis was detected. A few days after the replacement of the blood lost, this symptom ceased. The tracheostoma was removed 20 days after the insertion, and the patient was discharged to her home 33 days after the surgical intervention. Recommendations made at that time were completed with the local treatment for the incipient sacral decubitus that appeared one month after the operation.
Discussion
The reported case shows how a giant abdominal mass can cause a sudden collapse of vital functions, intensified by suicidal drug use. Appropriate collaboration between the acute phase care providers, the psychiatrist and the rehabilitation team finally resulted in good physical and mental recovery. For the prevention of these situations, careful screening and adequate treatment of psychological factors may be helpful.
Reviewing the literature, there are several case reports published on giant or huge ovarian masses.
Katke has concluded in his study that giant ovarian masses require resection because of the compressive symptoms. The preferred mode of intervention in case of a suspected malignancy is laparotomy to prevent perforation and spillage of the cyst into the peritoneal cavity [1].
Kuwahara et al. have presented the treatment of a huge ovarian cyst requiring the management of inferior vena cava syndrome, bleeding, abdominal competence, and cosmetic problems. The abdominoplasty of a case with the evacuation of 85 L of fluid was described [2].
In their study, Güraslan et al. have presented the case of a 61-year-old patient admitted with complaints of abdominal swelling and dyspnea. They performed aspiration on the cyst before the total excision, and finally an ovarian mass of 42.5 kg in weight was removed [3].
Patients with similar pathology also face the anesthesiologist team, due to difficult intubation, and life threatening cardiovascular and pulmonary complications. Kb et al. emphasize the role of a careful preoperative evaluation, and the maintenance of intraoperative hemodynamic and fluid management [4].
Tang et al. have concluded that the suicidal ideation associated with depression symptoms is common in patients having gynecological tumors, especially ovarian ones. Social support, coping strategies, such as confrontation and prevention may be helpful in impeding suicidal ideations in this population [5].
Acknowledgements
Not applicable.
Conflict of interest
The authors declare that they have no conflict of interest. There was no use of special funding for this study.
References
- Kattke RD. Giant mucinous cystadenocarcinoma of ovary. A case report and review of literature. J Midlife Health 2016; 7(1): 41-4.
- Kuwahara M, Taniguchi A, Yurugi S, et al. A case of abdominoplasty after removal of giant ovarian cyst. Plast Reconstr Surg Glob Open 2014; 2(8): e195.
- Güraslan H, Yaşar L, Ekin M, Kaya C, Cengiz H, Gonenc M. A successful management of a giant mucinous ovarian tumor with intraoperative controlled fluid aspiration, Eur J Gynaecol Oncol 2015; 36(5): 615-7.
- Kb N, Pt P, Shivanna S, Cvr M. Anaesthetic implications and management of a giant ovarian cyst. Clin Diagn Res 2014; 8(3): 170-1.
- Tang GX, Yan PP, Yan CL. Determinants of suicidal ideation in gynecological cancer patients. Psychooncology 2016; 25(1): 97-103.
Download Full Article
- Tibor Novák: Successfully treated case of a patient with giant benign ovarian tumor and suicide attempt (2017, Journal of Hungarian Obstetricians and Gynaecologists, PDF, 3 pages, English, 276KB)