LITERATURE - 2017, Journal of Hungarian Obstetricians and Gynaecologists
Decreasing depression and anxiety symptoms in pregnant women with imminent abortion by means of art therapy

Author: Dita Baumane-Auza, MD
Privat practice „APERTO”, Riga, Latvia
Current research int he world shows that 16% of women during pregnancy develop depression and anxiety symptoms resulting in complications during labour as well as foetal growth retardation. Art therapy is one of the ways to reduce depression and anxiety symptoms which are usually concomitant. Some research has been performed on the effect of art therapy on reducing depression and anxiety symptoms in pregnant women but none in Latvia. Correlation has been found between depression and anxiety symptoms and imminent abortion, and art therapy seems to be an effective method in preventing of imminent abortions and improving pregnant women’s emotional and physical health.
Keywords: depression, anxiety symptoms, art therapy
A woman’s health during pregnancy affects the proceeding of pregnancy, labour and newborn health. Analyzing the literature sources, based on the clinical research within the last five years, it has been revealed that antenatal depression and anxiety are related to pregnancy complications (preeclampsia), labour complications (miscarriage, preterm labour), and foetal developmental disorders (growth retardation, newborns of low weight, foetal death). Untreated antenatal depression and anxiety may later result in postnatal depression [1].
The incidence of depression symptoms and anxiety symptoms in pregnancy are 7-15% and 6-16% on average, respectively [2]. According to the World Health Organization (WHO) data, statistically significant depression symptoms are encountered in around 20% of pregnant women in the 3rd trimester. Anxiety during pregnancy has a harmful effect on the foetus, new-born, and can result in a series of pregnancy and labour complications [3].
Depression and anxiety in pregnancy are treated not only medically in many countries, but alternative methods are also applied such as psychotherapy, psychological counseling and art therapy [4].
Art therapy has been proven to help pregnant women with emotional problems by reducing anxiety, depression, fear of childbirth, and offering a much deeper understanding of becoming a mother [5]. Art therapy helps to raise one’s self-control, self-esteem and affection to the expected baby.
Studying the effect of visually plastic art therapy on depression and anxiety during pregnancy is an innovative approach as no such studies have been done yet. Though art therapy in Latvia is a comparatively new health care field (Cabinet of Ministers Regulations, March 24. 2009. Nr.268 and Cabinet of Ministers Regulations, May 18. 2010. Nr.461).
Aim of study
The aim of the study was to check whether art therapy can decrease depression and anxiety symptoms in pregnant women and whether they correlate to imminent abortion, as well as to test the sustainability of results in a month’ time.
A pre-test questionnaire with partially structured interview and document analysis of mother’s passport data of a woman’s health and pregnancy process, foetal development by ultrasonography data, assessment of high and low risks of gynaecological and obstetric pathologies were considered as inclusion criteria. 64 patients (study group n=32, attending 13 art therapy sessions; and control group n=32, not attending art therapy), age from 20 to 35 years, from the 12-28th gestation week with mild and moderately severe depression symptoms as well as anxiety symptoms were enrolled.
The investigate depression and anxiety symptoms, two methods were used:
- Self-assessment questionnaire of anxiety signs (STAI Form Y-1): State- Trait Anxiety Inventory, Spielberger, Gorsuch, Lushene, Vagg & Jacobs, and
- Beck Depression Inventory II (BDAII), Beck, Steer&Brown, 1996.
For data analysis, descriptive statistics (mean arithmetic, mode, median, standard deviation) and conclusive statistics (parametric statistical test – Student’s t-criterion) were used.
The Rīga Stradiņš University Ethics Committee authorized the research, and the participants gave their informed consent.
General description of depression
Depression is present in about 5–10% of the population and 20–30% of chronic patients. It is twice as common in women as in men, and is diagnosed late (>5 years) in about 30% of the cases. An identical rate of incidence was found in pregnant women. The most frequent symptoms are low-depressive mood, no joy for life, lack of interests, increased tiredness, being in a sad or fearful mood, having hypochondriac complaints, sleep and appetite disorders, or headaches [6].
Beck’s cognitive approach includes the cognitive triad [7] – negative self-esteem, negative assessment of the presence or the environment and negative assessment of future [8] as well as thinking schemes (they start to develop in childhood and later on one’s personal experience, as well as identify oneself with the closest people around and it ends with the formation of new values and convictions) and wrong thinking (wrong processing of information) (Figure 1).
According to Bech et al., depression is characterized by a series of cognitive disorders due to the very patient’s assumptions such as: generalization, a sense of guilt, self-incrimination, exaggeration and dichotomic thinking [9].
![Figure 1. Cognitive triad and its influence on the manifestation, effects and motivations of depression [8]](/img/literatures/2017-01-decreasing-depression-and-anxiety-symptoms-in-pregnant-women-with-imminent-abortion-by-means-of-art-therapy/figure-1.png)
General characteristics of anxiety
Anxiety is seen in 25% of the total population regardless of their health [10]. Anxiety may be a symptom of the disease (e.g., depression) or a risk factor in the pathogenesis of a medical condition [11]. The biochemical markers increase in the pituitary and the adrenal glands ACTH (adeno-corticotropic hormone), cortisol, glucocorticoids; in serum: cholesterol, and triglycerides. During anxiety the gene activity also changes. Due to the stressors, the changes occur in the nervous system which further on coordinates fear-related sympathetic stimuli, which are manifested as emotional and physical symptoms [6].
Beck identifies anxiety as motivating symptoms (to be as far away from the traumatising situation as possible), affective of emotional symptoms (subjective feelings towards danger) and behavioural symptoms (accelerated thinking or speaking) as well [12].
There symptoms also indicate the patient’s worries about danger manifesting as oppressive conservative, involuntary “automatic thoughts” (verbal and visual manifestations), and the contents of which make physical and mental harm possible. These thoughts come on regularly and occur from the information processing system, which is activating the affects.
Izard identifies anxiety as the combination of emotions, in which fear is a dominating correlation of emotions and fear with several other fundamental emotions, such as suffering, anger, sense of guilt, shame and interest [13]. Fear is characterized by specific physiological changes, expressive behaviour and specific experience, which is formed from the perception of fear or a dangerous situation. The relationship of anxiety with moral evaluation and anger control are included into Spielberger’s Anxiety Inventory measuring anxiety as a personality trait or anxiety (T trait), and anxiety as situative anxiety (emotional reaction to threat) or anxiety phase (T phase) [14].
Characteristics of depression and anxiety in pregnant women
During pregnancy, these disorders are seen in about 40% of women [15]. Depression symptoms have been seen in 7.4% of the cases in the first trimester, 12.8% in the second trimester, and 12% in the third trimester, which can be explained by neuroendocrine changes in the brain influencing the foetus, crossing foetoplacentar barrier [16, 17].
The risk of developing depression is essentially higher in teenage or early adolescent pregnancies. Depression is also encountered in patients with affective illnesses, and depression in the family history or in the obstetric history of the woman [11].
On the one hand, central neural and endocrine changes during pregnancy are physiological and mobilize the woman’s body for pregnancy; on the other hand, similar neuroendocrine changes have also been seen in anxiety and depression cases as a result of external and internal irritations. Both in anxiety and in pregnancy, the pituitary gland intensively secretes ACTH, and the adrenal glands cortisol, glucocorticoids, mineral corticoids, renin and angiotensin. This is the reason why the woman during pregnancy is more exposed to signs of depression and anxiety [4]. Changes take place in the limbic system, viscerosomatoemotional reactions, which are manifested as mood changes, taste changes, fear and uncertainty as to the expected pregnancy and its outcome [6].
Antenatal depression is seen in 7–20% of pregnant women, and if untreated, it may leave after-effect on the woman’s whole further life, being the greatest risk factor for postnatal depression and postnatal psychosis. Antenatal depression and anxiety are often combined. 27% of the women in the first trimester feel tired and have sleep disorders which are connected with the oestrogen level changes, frequent urination, leg cramps, breathing prob-lems, nausea and vomiting. Tiredness, nausea and vomiting are connected to depression and inability to do mental and physical work. These factors initiate a greater risk for preeclampsia and pre-term labour. Many authors in their studies indicate to The direct relationship between depression and increasing nausea and vomiting is suggested [18, 19], as well as the fact that antenatal stress, anxiety and depression cause pre-term labour risk, foetal retardation, and low birth weight, and low Apgar scores (<8) [20]. Increased anxiety and depression increase foetus activity and decrease foetal development as early as the 20-22nd gestation weeks [21].
Depression and anxiety symptoms should be differentiated from pregnancy-related symptoms such as tiredness, loss of appetite and energy, and cases of anaemia and hypothyroidism [11]. Some authors refer to negative emotions of women in pregnancy: unexplained fear of pregnancy complications, separation anxiety after delivery, fear of the expected delivery, fear of conventional Caesarean section, fear of not being able to cope with the newborn, shame and disappointment of the body changes during pregnancy, internal fight between the feminine and motherly side, aggressive fantasies against the still unborn child [23]. Quite often the reasons for depression and anxiety symptoms lie in the relationship of the couple, or employment and socio-economic factors.
Nevertheless, antidepressants should be administered very carefully because they cross the placentary barrier and are potentially teratogenic. Therefore, pregnant women are advised to use alternative methods to decrease anxiety, for instance, art therapy [4]. Art therapy activates the parasympathetic nervous system, interrupting sympathetic impulses and, as a result, decreasing sympathetic nervous system reactions [24]. It facilitates positive emotions stimulated by dopaminergic and opioid systems, stimulating positive effects.
Theoretical approaches in art therapy to overcome depression and anxiety
Since art therapy has been used in pregnancy only for a short term, most commonly directive techniques and structured tasks are applied to change and overcome anxiety and fear [28, 26], e.g. drawing fear and overcoming fear, the woman is focusing on personal conflicts much deeper, which requires attention and solution, while transformation allows the woman to look at the situation from a different angle, which has seemed to be negative so far [5]. Self-portrait, in its turn, can be used as a directive task for the adaptation towards the new role – the role of mother and accepting her own new body’s image.
Freud’s unconsciousness theory in art therapy became the basis for further psychoanalytical/psychodynamic approach in art therapy recognizing the unconsciousness of patients’ fantasies, daydreams and fears, and project them in pictures much faster than by words. Jung’s active imagination technique and amplification method are quite often used: free associations, spontaneous drawing and scribbling techniques. Spontaneously created piece of work in art therapy makes access to subconsciousness, through creative self-expression revealing one’s thoughts and emotions [27].
Art therapy in pregnant women makes us possible gain a deeper understanding of the woman’s new role as a mother, transforming fear into the ability to become a mother [26]. Self-portrait for the future through creativity encourages the increase of one’s self-esteem and dignity [30].
Methods
Initially, when doing the group selection, the descriptive statistical indices were calculated for two independent selections of pregnant women study group (I1) (n=32) and control group (K1) (n=32). Prior to it, by means of Kolmogorov-Smirnov Z criterion, we checked whether the empirical distribution of signs to be studied corresponded to the normal distribution of the study group (I1) (n=32) and control group (K1) (n=32) before the art therapy (Table 1) and after it (Table 2).
| Table 1. Study group (I1) (n=32) and control group (K1) (n=32) Measurement 1 | ||||||
|---|---|---|---|---|---|---|
| Measurement 1 | ||||||
| Study group (I1) (n=32) | Control group (K1) (n=32) | |||||
| T-status | T-sign | BDA II | T-status | T-sign | BDA II | |
| Kolmogorov-Smirnov Z criterion | 0.846 | 0.739 | 0.909 | 0.578 | 1.270 | 0.940 |
| Significance (2-tailed) | 0.471 | 0.645 | 0.380 | 0.892 | 0.079 | 0.340 |
| p>0.05 there is conformity to normal distribution | ||||||
| Table 2. Study group (I2) (n=30) and control group (K2) (n=30) Measurement 2 | ||||||
|---|---|---|---|---|---|---|
| Measurement 2 | ||||||
| Study group (I2) (n=30) | Control group (K2) (n=30) | |||||
| T-status | T-sign | BDA II | T-status | T-sign | BDA II | |
| Kolmogorov-Smirnov Z criterion | 0.706 | 0.751 | 0.874 | 0.618 | 1.222 | 1.008 |
| Significance (2-tailed) | 0.702 | 0.626 | 0.430 | 0.840 | 0.101 | 0.262 |
| p>0.05 there is conformity to normal distribution | ||||||
The frequency distribution of the studied signs of depression and anxiety (T-status and T-signs) corresponded to the normal distribution as the Kolmogorov-Smirnov Z criterion significance was higher than 0.05. Further on, t criteria were calculated for independent selections and hypothesis defined on similarity of both selections.
After conclusion of 13 sessions of art therapy cycle in the study group, the second measurement was done STAI Form Y-1 and BDA II questionnaire in the study group and the control group. Statistical calculations were done using descriptive and conclusive statistics for the data analysis.
A month after art therapy, the third measurement was done STAI Form Y-1 and BDA II questionnaires in the study group to assess the stability of results (due to subjective reasons, 4 respondents did not participate in this measurement). It did not show statistically significant difference from the 2nd measurement.
Descriptive statistics were used for data analysis and conclusive statistics (t criterion). Data were processed in SPSS program.
Statistical analysis
Statistical calculations were performed on statistically significant differences in the study group results before and after art therapy, and in the control group results before and after art therapy in the study group in the depression symptom scale, T-status and T-signs scales (Table 3).
There were significant differences between depression and anxiety symptom indices in pregnant women in the study group before and after their participation in art therapy. There were statistically significant differences in the study group between anxiety symptom indices of T-status indices (t=5.634; p=0.000) before and after art therapy, and depression symptom indices before and after art therapy in the study group (t=5.664; p=0.000) (Table 3).
| Table 3. Comparison of mean indices of anxiety and depression symptoms before and after art therapy | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Dependent selections | T-status | T-sign | BDA II | ||||||
| χ | t | A | χ | T | A | χ | t | α | |
| I1 | 42.3750 | 5.634 | 0.000 | 43.2500 | 6.361 | 0.000 | 19.1250 | 5.664 | 0.000 |
| I2 | 28.5000 | 31.0667 | 10.7000 | ||||||
| K1 | 42.1875 | -0.056 | 0.956 | 43.3125 | -0.238 | 0.813 | 18.5000 | 0.041 | 0.968 |
| K2 | 42,3333 | 43,8667 | 18,4333 | ||||||
| p<0.05 there is statistically significant difference between the mean indices of selections | |||||||||
| Table 4. Comparison of mean indices of depression and depression symptoms after art therapy | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Independent selection | T-status | T-sign | BDA II | ||||||
| χ | t | A | χ | T | α | χ | t | α | |
| I2 | 28.5000 | 5.935 | 0.000 | 31.0667 | 6.032 | 0.000 | 10.7000 | 5.264 | 0.000 |
| K2 | 42,3333 | 48,8667 | 18,4333 | ||||||
| p<0.05 there is statistically significant difference between mean indices of selections | |||||||||
As seen in the summary of the study results, there were statistically significant differences between depression and anxiety symptom indices in pregnant women in the study group after art therapy, and in the control group, in the second measurement after participation of the study group in art therapy. The study results show that there were statistically significant differences after art therapy in the study group and in the control group second measurement between anxiety symptom indices of T-status indices (t=5.935; p=0.000), anxiety symptom indices of T-signs indices (t=6.032; p=0.000) and depression symptom indices (t=5.264; p=0.000) (Table 4).
There was a positive, statistically significant correlation between imminent abortion, anxiety and depression symptoms, which may prove that all study participants who had an imminent abortion also had depression and anxiety symptoms (Table 5).
- There was statistically significant correlation between the threat of pregnancy interruption, anxiety and depression level. If there was a threat of pregnancy interruption, there was higher anxiety level (T-status, T-sign) and depression level (BDAII).
- There was also a tendency of statistically significant positive correlation between pregnancy toxicosis and anxiety level (T-sign) (p=0.053), which may mean that patients with pregnancy toxicosis were seen to have higher anxiety level (T-sign).
In order to check the stability of the study results, statistical calculations on statistically significant differences were done in the study group a month after art therapy session on depression symptom and anxiety symptom (T-status and T-sign) scales (Table 6).
| Table 5. Correlation of the results of Beck Depression Inventory II (BDAII), Self-assessment questionnaire with negative experience in previous childbirth, pregnancy toxicosis in present pregnancy and threats of pregnancy interruption in present pregnancy in the study and control groups before art therapy (n=64) | ||||
|---|---|---|---|---|
| T-status | T-sign | BDA II | ||
| Preterm delivery | Pearson Correlation | 0.209 | 0.182 | 0.207 |
| Significance | 0.097 | 0.150 | 0.100 | |
| N | 64 | 64 | 64 | |
| Pregnancy toxicosis | Pearson Correlation | 0.194 | 0.243 | 0.287 |
| Significance | 0.125 | 0.053 | 0.021 | |
| N | 64 | 64 | 64 | |
| Pregnancy interruption threats | Pearson Correlation | 0.343 | 0.388 | 0.352 |
| Significance | 0.006 | 0.002 | 0.004 | |
| N | 64 | 64 | 64 | |
| p<0.05 There is positive, statistically significant correlation if significance level is lower than 0.05 | ||||
| Table 6. Comparison of mean depression and anxiety indices in comparison to results in the study group after art therapy and a month after art therapy | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Dependant selections | T-status | T-sign | BDA II | ||||||
| χ | t | A | χ | T | A | χ | t | α | |
| I2 | 28.5000 | -0.981 | 0.331 | 31.0667 | -0.529 | 0.599 | 10.7000 | -0.273 | 0.786 |
| I3 | 30,4615 | 32,1923 | 11,0769 | ||||||
| p<0.05 there is statistically significant difference between mean indices of selections | |||||||||
Discussion and conclusions
The research results confirmed that depression and anxiety symptoms in the study group statistically significantly reduced after art therapy (2nd measurement, Table 3). Stability of results was preserved even a month after art therapy (3rd measurement, Table 6). The 1st and 2nd measurements showed statistically insignificant differences in both aspects in the control group (Table 4), which can be explained by the fact that no art therapy was performed in this group.
In pregnant women, both anxiety and depression symptoms were present. Thus, it was important to include some tasks into the art therapy plan which would help them identify and correct distorted conceptual schemes and dysfunctional conceptions, teach them to fix their negative automatic thoughts, understand and judge how they would affect their feelings and health. It was important for pregnant women in the study group to solve emotional difficulties, which were in the background of depression and anxiety. Support therapy for the coordination of one’s psychological needs by promoting perception changes of anxiety and fear goes hand in hand with one’s self-transformation, self-development process, and improvement of communication skills and acceptance of one’s body image. Using the cognitive behavioural approach is beneficial by the integration through the prism of humanistic and psychoanalytical approach, directive techniques and structured tasks with an aim to change and overcome anxiety and fear perception, consequently influencing causative relationship of anxiety and depression.
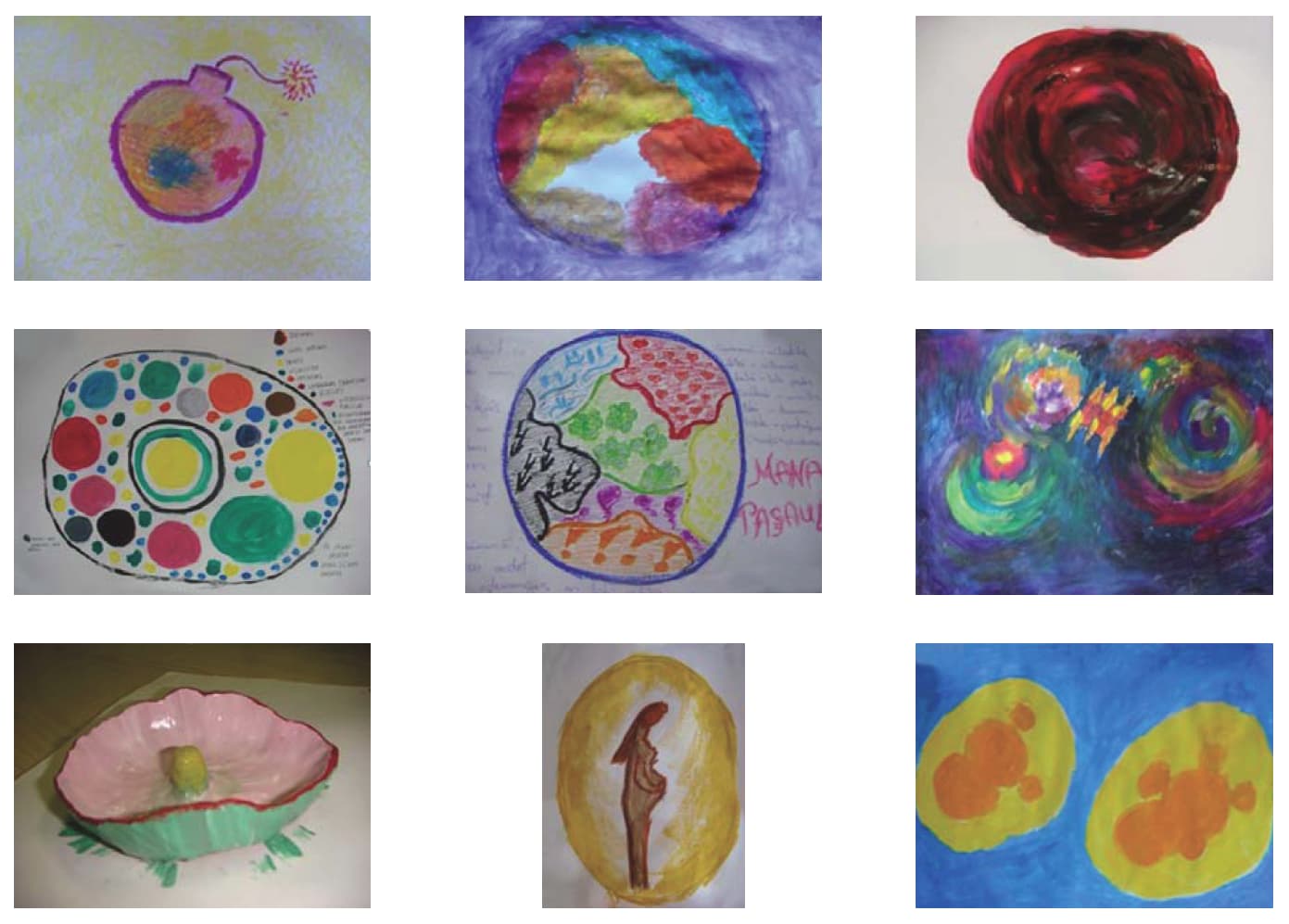
At the initial stage of art therapy, pregnant women’s emotions were suppressed, marked control dominated over their behavior and the created piece of art. The participants were worried that the evaluation of their work by other women could be negative. Signs of anxiety could be identified in the choice of colours (mostly dark) and forms, primitive lines. At the conclusive stage of art therapy, with the lessening of depression and anxiety symptoms, women became more relaxed, used brighter colours; the drawing covered a comparatively larger part of the sheet indicating a more positive perception of oneself and their future.
Warm-up exercises, the use of different materials of art stimulated the creativity level of the participants, and first of all, helped them relax at the kinetic-sensation level. With the decrease of perception control, they got more actively involved into art therapy focusing their attention on it. Comparing this stage with that of the beginning, the images and symbols in art therapeutic activity were depicted in multidimensional work, richer both in form and means of expression, going deeper and focusing on the understanding of the created work. Using one’s individual creativity, each woman learned more about herself and the potential of group communication and spontaneity. The aim of the task was to focus on colours and forms, how they were reflecting the women’s mood. The perceptively-affective level being activized, the women tried to find representation for their internal and external experience, which helped them release their previously suppressed emotions. Representation of one’s own image, in connection with one’s own judgement about oneself, initiated associations and discussions how one’s body image is perceived and accepted. Recognition of emotions and their depiction helped the women understand their negative automatic thoughts, communication and behaviour types in relationship with other people. Many participants expressed dislike to themselves and their body changes during pregnancy. Having discussions and paying attention to each participant’s feelings and emotions, encouragement and support helped them relax and get rid of control, to accept the negative emotions as well, to understand oneself and the problems much deeper.
In the process of art therapy, it was important to broaden the patients’ space of life, creating larger scope of symbolic imagination, for instance, spontaneously created pieces of art (scribbling, drawing with a non-dominant hand, monotyping) created access to the subconsciousness, revealing thoughts and emotions through creative self-expression. Drawing by the non-dominant hand caused thoughts on situations of life changes, in case there were some limitations or losses. Using one’s active imagination and creativity, using different materials of art, and short warm-up exercises, helped pregnant women express thoughts and feelings of the moment and also the experience by working in a group. It helped the group dynamics because it caused frankness and sharing one’s feelings and emotions with the other groupmates. Freely chosen types of art expression, the factor of therapeutic relationship (triangular relationship, quality of therapeutic relationship, spontaneity, and creativity), the factor of reflexion and feedback strengthened the effectivity of using art therapy in the group work to overcome depression and anxiety symptoms.
At the stage of evaluation, participants were much deeper reflecting at the cognitively-symbolical level, focusing on negative automatic thoughts, changing the thinking schemes, turning attention to problem solving, the ability to plan perception of their image and future. Lusebrink’s concept on gradual expression levels of art is confirmed in relation to the use of art materials and technologies, and depict the development of patients’ mental and artistic manifestations, starting from spontaneous reactions till abstract and symbolic thinking [31]. Sometimes nonverbal communication with one’s own piece of art and nonverbal experience in the group was so strong that the created symbols were encountered in the pieces of art repeatedly (Jung defines them as “sparkling symbols”) [32], helping to identify internal conflicts, fear and worries, as well as to recognize oneself.
In the fifth session, the task for the group was to show „how I struggle with negative emotions and who helps me overcome them”. It was a dynamic turning point to see the resources at work with negative emotions to develop cooperation and to make new behavioural models. Depiction of emotions and physical feelings in a group work facilitated their mutual interactivity, communication, trust and emotional support in solution of common problems, as well as in looking for solutions of individual problems. At the same time, the ability of other participants to express their emotions and feelings created a sense of support, strengthened safety and self-confidence.
Creative process and therapeutic relationship characterize the efficacy of art therapy working process, depicting therapeutic changes from the patients’ point of view. Patients became livelier, more relaxed, more confident, could tell what they wanted, could ask for support when it was needed, could explain their emotions and verbalize them, could accept their negative emotions and their causes as well, could structure their needs, could devote more time to themselves, began to understand their problems and causes, could perceive different life situations much calmer, dared to express their ideas in the group, became calmer and more secure about themselves and the expected baby’s health, became less worried of the expected childbirth.
At the evaluation and conclusion stage of art therapy, the ability of pregnant women to understand their own and other people’s emotional reactions, behaviour was also increased, which helped them to learn, understand and perfect one’s own personality, behaviour, relationships, and internal resources.
Analyzing the group results statistically, first of all, attending the art therapy significantly changed the participants’ daily life by devoting some time only to themselves. Art therapy with its humanistic approach emphasized self-awareness, initiated the development of one’s capacities, self-assessment, creativity development and thinking of issues related to one’s own self (fear, anger, death, suffering, freedom).
Secondly, the aim of art therapy was to change the perception of anxiety and fear, interrupting automatic thoughts, changing wrong thinking and behavioural models. By this change, their behaviour was changed as well, which was reflected in a sense of greater safety, self-confidence, accepting one’s self-image, and the primary therapeutic aim – decreasing of depression and anxiety symptoms.
Thirdly, art therapy improved pregnant women’s communication skills. Doing repeated measurements a month after art therapy in the study group, the measured level of depression and anxiety showed stability of the acquired results.
Fourthly, it would be sensible to have cooperation between gynaecologists and obstetricians, family physicians and midwives offering art therapy as an essential additional method for depression and anxiety symptoms in pregnant women, as it could significantly improve pregnant woman’s health and the health of the new-born, as well as the outcome of childbirth (Figure 2).
BIBLIOGRAPHY
- Alder Judith, Fink Nadine, Bitzer Johannes, Hösli Irene,& Holzgreve Wolfgang, (2007) Depression and anxiety during pregnancy: A risk factor for obstetric, fetal and neonatal outcome? A critical review of the literature. The Journal of Maternal – Fetal and Neonatal Medicine March 2007; 20(3): 189-209.
- Janice H, Goodman, Tyer-Viola Lynda. Detection, Treatment, and Referral of Perinatal Depression and Anxiety by Obstetrical Providers. Journal of Women’s health 2010; 19(3): 477-490.
- WHO mhGAP. Intervention Guide for mental, neurological and substance use disorders in non-specialized health settings. WHO; 2021.
- Bauer M, Berghöfer A, Adli M. Akute und therapieresistente Depressionen. Verlag Heidelberg: Springer Medizin; 2005. p. 118-121.
- Swan-Foster N. Images of the pregnant woman: Art therapy as a tool for transformation. The Arts in Psychotherapy 1989; 16: 283-292.
- Klußmann R, Nickel M. Psychosomatische Medizin und Psychotherapie, Ein Kompendium für alle medizinischen Teilbereiche, 6. Auflage. Wien: Springer-Verlag; 2009. 12 p. 301-302.
- Классен ИА. Практическая психотерапия .Москва МЕДпрессинформ; 2004. p.328-335.
- Beck T. Aaron, Alford A. Brad. Depression. Causes and Treatment, University of Pennsylvania Press; 2009. pp. 8-17; 214-245.
- Beck T. Aaron, Rush A. John, Shaw F. Brian, Emery Gary. Cognitive therapy of depression. New York: Published by The Guilford Press; 1979. p. 261.
- Kessler RC, Sonnega A, Bromet E, et al. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995; 52: 1048-1060.
- Levenson JL. Textbook of Psychosomatic Medicine. Washington, DC: London, England; American Psychiatric Publishing, Inc.; 2005. pp. 251-253, 742-744
- Beck T. Aaron, Emery Gary. Anxiety disorders and phobias. USA: Published by Basic Books; 2005. pp. 4, 31, 103, 167.
- Izard CE. Anxiety: a variable combination of interacting fundamental emotions. In: Spielberger CD. (ed.). Anxiety. Current Trends in Theory and Research. New York: Academic Press; Vol. 1. 1972.
- Spielberger D. Charles, Sarason G. Irwin. Stress and Emotion. Anxiety, Anger and Curiosity, Routledge Taylor&Francis Group; 2005. pp. 20-25, 47, 98-102.
- Kelly RH, Zatzick DF, Anders JF. The detection and treatment of psychitraic disorders and substance use among pregnant women cared for in obstetrics//Am 3 Psychiar 2001; 158: 213-219.
- Shuang Ji, Qi Long, Newport D, Jeffrey, Hyeji Na, Knight Bettina, Zach B. Elizabeth, Morris J. Natalie, Kutner Michael, Stowe N. Zachary. Validity of depression rating scales during pregancy and the postpartum period: Impact of trimester and parity. Journal of Psychiatric Research 2011; 45: 213-219.
- Tarayn G. Fairlie, Matthew W. Gillman, Jane Rich- Edwards. High Pregnancy-Related Anxiety and Prenatal Depressive Symptoms as Predictors of Intention to Breastfeed and Breatfeeding Initiation: Journal of Woman’s health 2009; 18(7): 945-953.
- Andersson L, Sundstrom-Poromaa I, Wulff M, Astrom M, Bixo M. Implications of antenatal depression and anxiety for obstetric outcome. Obstetric and Gynecology 2004; 104: 467-476.
- Gülengül Köken, Mehmet Yilmazer, Emine Cosar, Figen Kir Sahin, Serhan Cevrioglu, & Ömer Gecici. Nausea and vomiting in early pregnancy: Relationship with anxiety and depression, Journal of Psychosomatic Obstetrics& Gynecology June 2008; 29 (2): 91-95.
- Berle JØ, Mykletun A, Daltveit AK, Rasmussen S, Holsten F, Dahl AA. Neonatal outcomes in offspring of woman with anxiety and depression during pregnancy. Arch Womens Mental Health 2005; 8: 181-189.
- Conde A, Figueiredo B, Tendais I, Teixeira C, Costa R, Pacheco A, Rodrigues MC, Nogueira R. Mother’s anxiety and depression and associated risk factors during early precnancy: effects on fetal growth and activity at 20-22 weeks of gestation. Journal of Psychosomatic Obstetrics and Gynaecology Jun 2010; 31 (2): 70-82.
- Misri Shaila, Kendrick Kristin, Oberlander F. Tim, Norris Sandhaya, Tomfohr Lianne, Zhang Hongbin, Grunau E. Ruth. Antenatal Depression and Anxiety Affect Postpartum Parenting Stress: A Longitudinal, Prospective Study. Psychiatry 2010; 55(4): 222-228.
- Hocking L. Kimberly. Artistic narratives of self-concept during pregnancy. The Arts in Psychotherapy 2007; 34: 163-178.
- Hass-Cohen N, Carr R. Art Therapy and Clinical Neuroscience. London and Philadelphia: Edited by Noah Hass-Cohen and Richard Carr. Jessica Kingsley Publishers; 2008.
- Hogan S. A discussion of the use of art therapy with woman who are pregnant or who have recently given birth. In S. Hogan (Ed.) Gender issues in art therapy. London: Jessica Kingsley; 2003. pp. 148-172.
- Swan-Foster N, Foster S, & Dorsey A. The use of the human figure drawing with pregnant woman. Journal of Reproductive& Infant Psychology 2003; 21(4): 293-307.
- Rubin Judith Aron. Approaches to Art Therapy: Theory and Technique, Second Edition, New York: Brunner-Routledge; 2001. pp. 15-326.
- Hogan S. Art therapy and Anger. Marian Liebmann; 2008. pp. 198-200.
- Malchiodi A. Cathy. Handbook of Art therapy. New York; 2003. pp. 41-92.
- Buchalter I. Susan. A Practical Art Therapy. London and Philadelphia: Jessica Kingsley Publishers; 2004.
- Lusebrink VB. Assessment and therapeutic applications of the predominant levels of the Expressive Therapies Continuum: Theoretical implications involving brain structures and functions. In: Art Therapy Journal of the American Art therapy association. 2010.
- Jung C, Read H, Fordham M& G. Adler (Eds.) Bollingen series XX: The collected works of C.G. Jung. New York: Pantheon Books; 1959. p. 102.
Download Full Article
- Dita Baumane-Auza: Decreasing depression and anxiety symptoms in pregnant women with imminent abortion by means of art therapy (2017, Journal of Hungarian Obstetricians and Gynaecologists, PDF, 8 pages, English, 240KB)