LITERATURE - 2016, Journal of Hungarian Obstetricians and Gynaecologists
The Forceps - From Oblivion to Necessity

Author: Petru Chitulea
University of Oradea, Faculty of Medicine and Pharmacy, Department of Obstetrics and Gynaecology, Oradea, Romania
Across the centuries, obstetricians have looked for methods and instruments to extract the fetus from the pelvic genital tract when natural birth was impossible. A wide variety of forceps have been created, which are mostly used today, such as the Tarnier forceps, the Naegele forceps, the Kjelland forceps, and the Simpson forceps. The forceps is used in all the clinics of the world as a saving instrument when the fetus’ life or the mother’s life is in danger due to acute complications of the expulsion time that have not been foreseen. The three major modern indications for forceps usage are: the labor’s failure to progress, fetal distress in expulsion, and maternal distress are still valid. “Darkness creates monsters” – defying the saving role of the forceps and the way in which it works produces fear – both to women in parturition and unadvised obstetricians. This is why educating, firstly the residents – about the advantages and the technique of using the forceps – but also the pregnant women in the Mother’s School – on the saving role the forceps on their child – should become a rule.
Keywords: forceps, fetal distress in expulsion, application of forceps
The iconic instrument of the 19th century until mid-20th century obstetrics, the forceps, has fallen into oblivion in the last decades being eliminated almost entirely from the current obstetrics practice. This is in primarily due to the general public’s misunderstanding of forceps, which led to the new generation of obstetricians with little experience using the tool, and therefore many doctors choose to perform cesarean surgery instead of using forceps.
The mere utterance of the word “forceps” brings goose-bumps among the women in parturition in the delivery room. The instrument gained its sinister reputation, mostly unjustified, in the 19th century and the first part of the 20th century when it was used instead of the cesarean surgery. However, it is actually a ‘saving’ instrument.
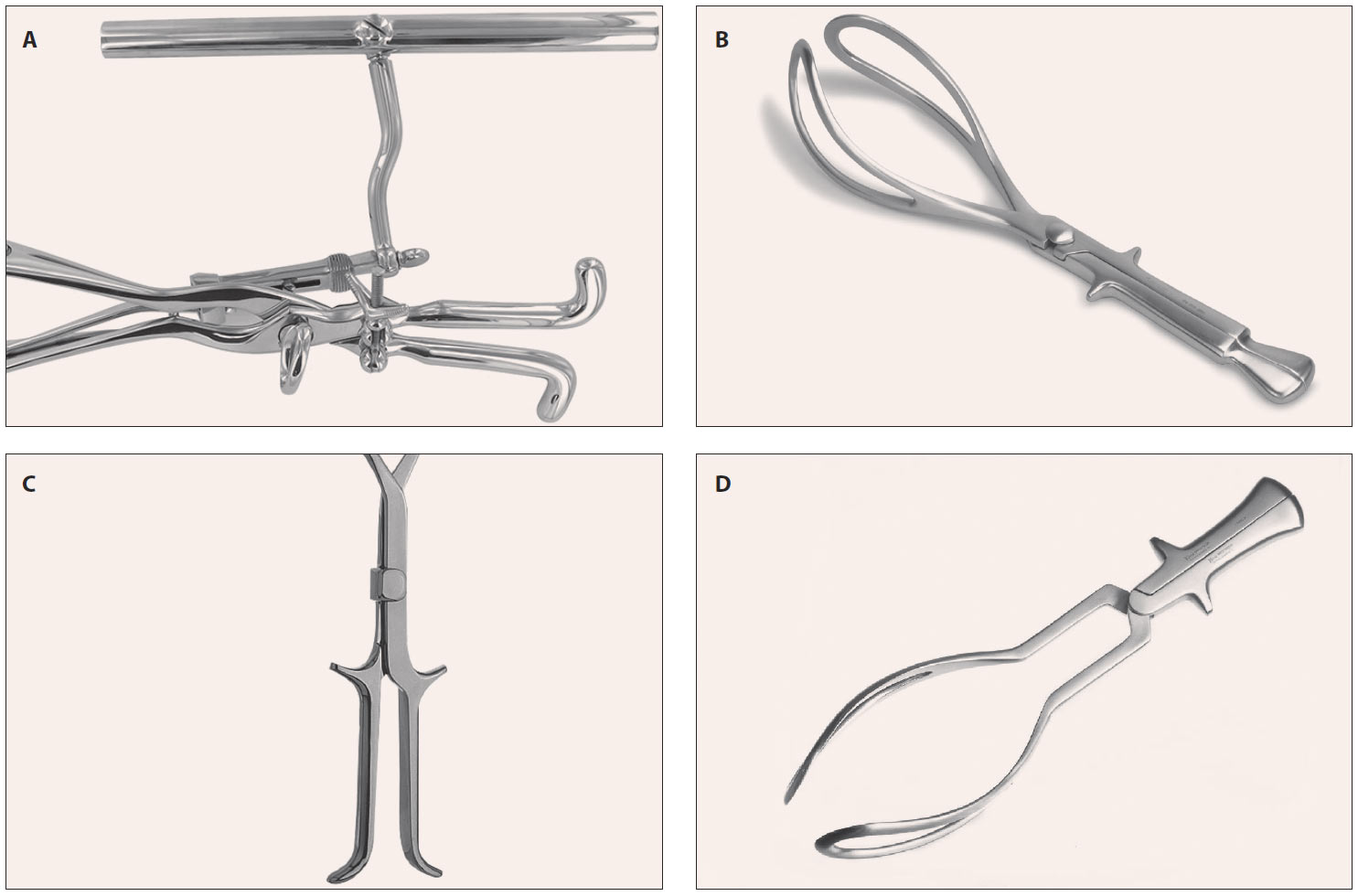
Across the centuries, obstetricians have looked for methods and instruments to extract the fetus from the pelvic genital tract when natural birth was impossible. Many instruments have been created starting from Antiquity to the Middle Ages (Avicenna in the 10th century), Chamberlen Forceps in the 18th century, until the golden age of forceps in the 19th century. A wide variety of forceps have been created, which are mostly used today, such as the Tarnier forceps, the Naegele forceps, the Kielland forceps, and the Simpson forceps (Figure 1.).
In the last decades, the increased security of the cesarean surgery which, from Baudelauque’s ‘murderous surgery’ has become a very clearly documented procedure – simple, rapid, and secure – and has eliminated a series of obsolete procedures on the usage of the forceps. Despite all of these factors, the forceps is used in all the clinics of the world as a saving instrument when the fetus’ life or the mother’s life is in danger due to acute complications of the expulsion time that have not been foreseen. With the unprecedented development of the investigation methods in perinatal obstetrics and medicine (ultrasound, Doppler flow meter etc.) a great number of dramatical “surprises” from the expulsion have been foreseen and thus, corrected in time or they have been resolved through the cesarean surgery. In an ideal world where all pregnant women are being monitored regularly, appropriately and rigorously, the forceps usage would be pointless. However, since the obstetrics is far from this ideal situation, the cases of pregnant women brought to the emergency room of the maternity in labor – where they encounter for the first time an obstetrician – is not, unfortunately, a rarity. Therefore, the three major modern indications for forceps usage are: the labor’s failure to progress, fetal distress in expulsion, and maternal distress are still valid.
The labor’s failure to progress
In modern obstetrics, the labor’s failure to progress refers mainly to the expulsion period when, because of the vicious rotation of the fetal skull in the posterior varieties, fetopelvic disproportion (undetected in time), bone abnormalities or abnormalities of the soft tissue of the delivery canal undiagnosed, or the anesthesia administration used in the last decades, which inhibits the feeling of screaming, may lead to the blocking of the fetal skull in the excavation or in the inferior strait. In such situations, which represent the last part of a painful and slow labor, the decision to undergo a cesarean surgery may be risky because the abdominal extraction of the fetal skull – which is deeply engaged in the pelvis – is extremely traumatizing, both for the fetus and the mother. These may lead to fetal traumas and lesions and/or uterine lesions (the rupture of the inferior segment, or lateral towards the parameters, or sometimes anteriorposterior leading to bladder lesions) which lead always to a massive hemorrhage that may endanger the integrity or even the life of the patient.
This is the reason why the usage of the forceps and the process of extraction performed with it, in the above mentioned cases, is not only safer from a maternal-fetal standpoint, but it is faster and less traumatizing - assuming the usage of the forceps is correctly applied and at the right time. Besides, the bad reputation of the forceps comes from the cases in which it was used too late, when the fetal hypoxia and the consecutive biochemical trauma already occurred. The mechanical trauma of the forceps, which is minor (the pressure applied onto the fetal skull is between 2.5–3 kgf) is the last drop in the fetal drama (1, 2).
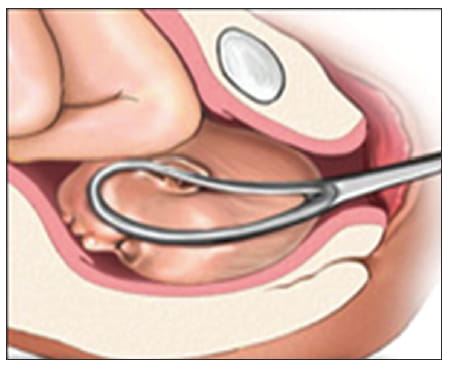
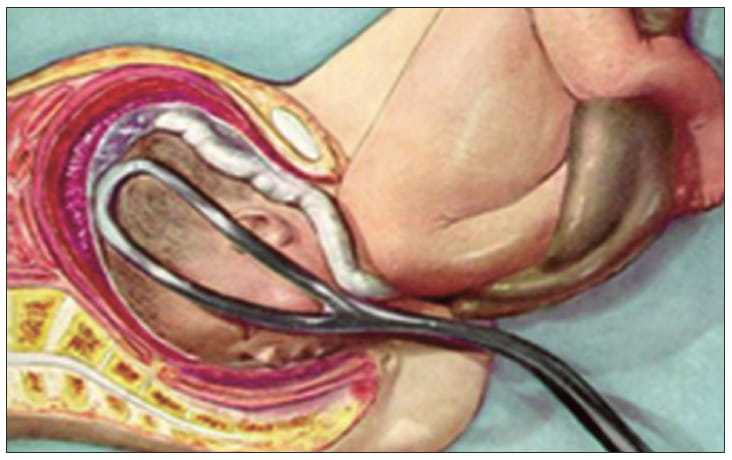
A last indication in this category is the blocking caused by the deflecting of the skull behind – in the case of pelvic breech – when after the delivery of the entire body, the skull is stuck in the superior strait – this is an extremely dramatic situation in obstetrics in which the caesarian surgery is not an option. In such situations, if the Mauriceaux maneuver fails, the only option is the usage of the forceps on the skull (1, 2) (Figure 2–3.)
Fetal distress
Acute fetal distress in expulsion may be caused by the cord pathology (nuchal cord or real cord knot, congenital short cord) undiagnosed. In these situations, after an eutocic labor, without any premonitory sign, the fetal bradycardia appears in the expulsion (sometimes extreme, “inexplicable”) and thus, it is useless and counterproductive to perform a cesarean surgery. When an acute fetal distress occurs in the expulsion, the time needed to prepare the operating team, as well as the preoperative preparation, lead to a 10-15 min delay that may prove fatal to the fetus; therefore, the caesarian surgery will lead to an intrapartum stillborn or a newborn with a low Apgar score, all causing bad consequences.
This situation is, in my opinion, the most important indication of the usage of the forceps – when the extraction of the fetus can be performed very quickly (approx. 1 minute) and the fastness of the procedure saves the fetal brain.
Maternal distress
Any maternal distress that requires the woman in parturition to not undergo the expulsive effort is an indication of the usage of the forceps. Therefore, heart diseases, pulmonary tuberculosis, a history in strokes, sometimes cicatricial uterus, plastic surgeries to the abdominal wall (hernias, eventrations) – they all may indicate the need to use forceps. In this category of indications we must highlight one of the classical indications, harder to define, i.e. maternal exhaustion – this overlaps with the indication of the labor’s failure to progress.
Moreover, the three categories of indications in the usage of the forceps, though different in didactic purposes, intertwine and overlap with each other. The decision to use the forceps, together with its timing, must be determined by an obstetrician with experience and clinical discernment.
The conditions in the usage of the forceps
Any forceps usage is done in the case of a living fetus. However, in the case of an intrapartum stillborn, the standard indication is: craniotomy, cephalotripsy, or embryotomy; they are all meant to reduce the dimensions of the fetus so as to avoid maternal trauma.
The second condition to the usage of the forceps is the precise diagnosis of presentation, position, and the variety of positions, and also the anatomic state of the delivery canal (a caesarian surgery is performed from the very beginning on a vitiated pelvis, the permeability of the pelvis, and also the soft tissue permeability – the complete dilation of the cervix) (1, 2).
The forceps in modern obstetrics – far from a sinister torturing tool – is a saving instrument in numerous cases in which the rapid extraction of the fetus from the pelvic genital tract is urgent. The usage of forceps and the extraction may be viewed as a success when the fetus has a minimum score of 8 on the Apgar scale. The purpose of the forceps usage is to protect the fetus from acute hypoxia developed during the expulsion. The fetal cortex is the most sensitive to hypoxia because it is the last phylogenetic acquisition of the human race, thus leading to irreversible neuronal death. The correct usage of the forceps is nontraumatic for the fetus. The compression force of the forceps is between 2 and 3 kgf, and the traction on the fetal neck should be of about 20 kgf (1, 2).
The usage of the forceps on the superior strait and the forceps used as a reducer of fetal skull dimensions have become obsolete. It must not be used in order to replace the cesarean surgery, but represents a saving obstetric maneuver in critical unexpected and unforeseeable situations. In the last decades, a large number of generations of obstetricians have been poorly trained in the usage of forceps, thus increasing the number of cesarean surgeries; the number increased on one hand, because of the legitimate broadening of its indications, and on the other hand, through the loss of the obstetricians’ abilities to perform obstetrical maneuvers.
The use of the forceps, like any other obstetrical and surgical maneuver, generally needs knowledge acquired thorough practice. Replacing the forceps with the cesarean surgery – which has been legitimate and reasonable in many ways – produced generations of well-trained obstetricians in is performance. But if they face emergency situations, they feel “unarmed” when it comes to the ability of correctly performing obstetrical maneuvers. The decreased number of forceps usage in obstetrics is also determined by the reluctance (legitimate in most of the cases) of the women in parturition who do not wish to deliver in this method, but also because of the media and legal pressure on the obstetricians.
Regardless of the causes, the consequence of this context is the fact that less obstetricians are capable to save the fetus in the case of an unexpected obstetrical emergency in the expulsion.
What is to be done?
“Darkness creates monsters” – defying the saving role of the forceps and the way in which it works produces fear – both to women in parturition and unadvised obstetricians. This is why educating, firstly the residents – about the advantages and the technique of using the forceps – but also the pregnant women in the Mother’s School – on the saving role the forceps on their child – should become a rule. Nowadays, in some of the maternities, in Mother’s School it is advertised that the maternity does not have any forceps; this is done to increase the trust of the pregnant women, while drawing them to that maternity. A well-informed pregnant woman should run as far away as possible from such a maternity. The old obstetricians said about the forceps that it is non vi sed arte, i.e. you do not need to use the force, but the obstetrical art. In modern understanding, solving an obstetrical emergency does not rely primarily on the medical instruments, nor on the hands of the obstetrician, but on his brain and his medical wisdom which should be used as much as possible.
Conflict of interest
The author declare no conflict of interest.
References
- Munteanu I. Tratat de Obstetrica, Editia a II-a, Volum I, Editura Academiei Romane; Bucuresti: 2006. Cap. 9.4. Aplicarea de Forceps, Baster G, Luca V. pg. 564–591.
- Alessandrescu D. et al, Probleme de Practica si Tehnica Obstetricala, Editura Medicala; Bucuresti: 1965. Cap. al VI-lea, Interventiile Obstetricale de Terminare a Nasterii A. Forcepsul pg. 283–321.
- Chitulea P, et al. Actualitati in Obstetrica si Ginecologia Secolului XXI, Editura Universitatii din Oradea: 2014. Forcepsul – Un instrument cazut in desuetitudine p. 19–25.
- Chitulea P. et al. Etiologia operatiei cezariene in secolul XXI – Tehnici chirurgicale moderne in cezariana, Editura Versa Media; 2016. Forcepsul – de la uitare la necessitate, p. 85–89.
Download Full Article
- Petru Chitulea: The Forceps - From Oblivion to Necessity (2016, Journal of Hungarian Obstetricians and Gynaecologists, PDF, 6 pages, English, 1MB)